Posted 9/04/18 in Valid Points, and on The Validation Institute’s blog.
“How many businesses do you know that want to cut their revenue in half? That’s why the health care system won’t change the health care system.”
Current Florida Governor and Former Columbia/HCA CEO Rick Scott at a 2012 Investor conference
 Health care management expert Fred Goldstein recently related an encounter with health system executives who acknowledged that their interest in improving two of the three Triple Aims – patient experience and health outcomes – did not extend to reducing the cost that drives their earnings. Similarly, several health system colleagues have recently disclosed to me their organizations’ lack of support for their Accountable Care Organizations and value-based contracting programs because, if managed properly, they reduce per patient revenues.
Health care management expert Fred Goldstein recently related an encounter with health system executives who acknowledged that their interest in improving two of the three Triple Aims – patient experience and health outcomes – did not extend to reducing the cost that drives their earnings. Similarly, several health system colleagues have recently disclosed to me their organizations’ lack of support for their Accountable Care Organizations and value-based contracting programs because, if managed properly, they reduce per patient revenues.
The worry that right-sizing US health care will yield less money for the health care industry is an obvious, powerful barrier to meaningful health care change. We’ve made relatively little policy progress toward that goal, and for all their protests about being on the side of better value, the industry has been absolutely clear that unnecessary care and irrational pricing are acceptable tools if they help them achieve their current financial goals.
The health care industry, Congress’ and legislatures’ most powerful lobby, has captured the regulatory process, so policy change that can force the issue is unlikely. And for all the talk about moving to paying for results and value-based care, fee-for-service still constitutes all but a tiny fraction of reimbursement arrangements.
Within the legacy system, decades of fee-for-service reimbursement have bloated virtually every procedure, rendering our care and cost patterns dramatically different than those in other countries. They, for example, have far lower percentages of specialists and a greater reliance on primary care. Per capita rates of expensive, common procedures, like imaging and coronary stenting, are a fraction of ours. The net results are generally better health outcomes at a per capita cost that is half of what we pay.
We know that in a system that pays for more activity, overtreatment is one of our biggest problems. But estimates of unnecessary and inappropriate care and cost are plagued by methodological challenges, including definitions of what constitutes waste, and have been all over the map. In a 2017 national survey, physicians reported that about 20 percent of all care, including about a quarter of tests, more than a fifth of prescriptions, and more than a 10th of procedures, is all waste. In domains like orthopedics, cardiology and oncology, there’s broad acknowledgment that significant percentages of care provide little or no value. A 2012 estimate by Berwick and Hackbarth suggested that 18-37 percent of all 2011 US health care spending was waste. A 2008 PwC study, The Price of Excess, came in at a breathtaking 54.5 percent, which is close to the aggregated real world results (and performance guarantees) of high performance health care companies.
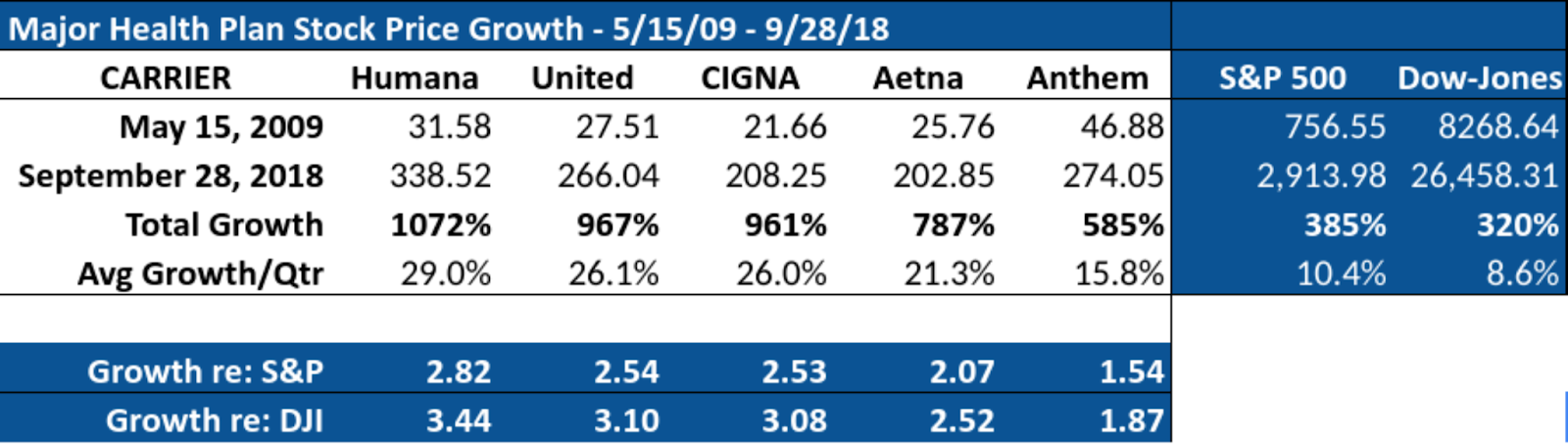
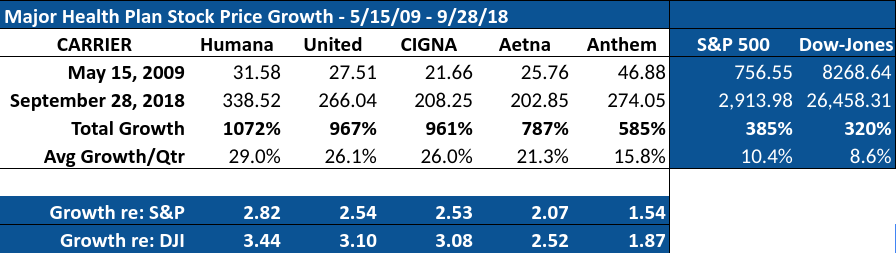
The health care industry has shown little interest in approaches that consistently deliver better health outcomes and/or lower cost. The awful subtext here is that egregious unit pricing and unnecessary/inappropriate care are not merely accidental byproducts of the US health system. Instead, health care companies’ business models have come to depend on those excesses. Their stockholders have become accustomed to extraordinary returns and, accordingly, their business strategies and tactics revolve around maintaining current and growing revenue streams. Delivering value around the right care is a dispensable nicety.
This is clear in the stock price growth of the major health plans. Humana and United have each grown about 1,000 percent over the past 37 quarters, which works out to a staggering average quarterly stock price increase of 28.4 percent and 26.0 percent, respectively.
So the US health care industry literally has a financial stranglehold on the American people that can capsize our social safety nets and our global competitiveness, destroying, as Dave Chase has so clearly described, the American dream. Large health care companies have aggressively lobbied Congress and the legislatures for years and own the policy environment. Their stock pricing prohibits intentionally rightsizing utilization and unit pricing. The prevailing model is toxic and can only lead to cataclysmic disruption, but the fix is in and they’re devoted to keeping it in place as long as possible.
Because, as a rule, health plans make more if health care costs more, they have little stake in approaches that would result in fewer services or lower costs. In that sense, they’re in a box that makes it difficult for them to drive higher value services, especially if that approach translates to reduced revenues and earnings. Upstart organizations and those relatively new to health care, like Amazon and Walmart, are not constrained by past financial performance or the imperative to maintain exorbitant stock prices.
Under these circumstances, coaxing health care organizations to do the right thing isn’t a promising scenario. A better path would be finding the rare scalable health care organization that has figured out how to consistently deliver superior results in high value niches, and that is willing to put its fees at risk with performance guarantees. Driving all the business within a domain – e.g., musculoskeletal care, cardiometabolic care, drug management, imaging management, claims review – to high value performers will erode the business to low- and mid-value performers and they’ll either hold out in hopes of saving the old paradigm or be co-opted. If it’s the latter, they’ll learn how to become practitioners of newer, more accountable, high performance approaches to clinical, financial or administrative health care management.
Our experience over the past several months, and discussions with a variety of progressive employers, unions and benefits managers, strongly suggests that we’re at the leading edge of a tipping point. I’m personally aware of groups representing more than 6 million covered lives that are actively engaged in going around their conventional health plan arrangements to implement high performance programs. A subset of that larger population will actually make the leap, of course, but the value proposition – better health outcomes at much lower cost now and into the future – is very compelling. The prospects are bright.
The message is that we’re not simply stuck with the status quo. There are solutions. Granted, during this early phase, the answers are more easily accessible to larger, self-insured employers than to smaller, fully insured groups, but as they gain traction, the better approaches will be available to everyone. And the possibility is very real that, by using the market, we can bring health care back to rights.
Brian Klepper is a health care analyst.
 A couple weeks ago a Journal of the American Medical Association article reported the results of a large (33,000 employees) rigorous study of worksite wellness programs. As explained in The New York Times, the research “found no significant differences in outcomes like lower blood pressure or sugar levels and other health measures. And it found no significant reduction in workers’ health care costs.”
A couple weeks ago a Journal of the American Medical Association article reported the results of a large (33,000 employees) rigorous study of worksite wellness programs. As explained in The New York Times, the research “found no significant differences in outcomes like lower blood pressure or sugar levels and other health measures. And it found no significant reduction in workers’ health care costs.” A class action legal ruling
A class action legal ruling A year ago,
A year ago,  It seems inevitable that, in the near future, an innovative health care organization is going to seize the market opportunity, gradually cobble all the pieces together, and demonstrate to organizational purchasers that it consistently delivers better health outcomes at significantly lower cost than has previously been available.
It seems inevitable that, in the near future, an innovative health care organization is going to seize the market opportunity, gradually cobble all the pieces together, and demonstrate to organizational purchasers that it consistently delivers better health outcomes at significantly lower cost than has previously been available. 
 In a recent
In a recent